



Ambulatory Acute COVID-19 Care Extends to Heart Failure Patients
New Risk Stratification and Advanced Protocols Allow Home Treatment

By Peter A. McCullough, MD, MPH
As a cardiologist, I have lost a few patients to acute COVID-19 respiratory illness and a key factor each time has been heart failure combined with a late start on early therapeutics. The hospital is too late to start treatment for acute COVID-19 in patients with left ventricular dysfunction. Palazzuoli et al have published an approach that focuses on optimal heart failure management and early COVID-19 therapy that allows management to be started in the home. Even if hospitalized, patients who receive standard of care multidrug home treatment are expected to survive the hospitalization.
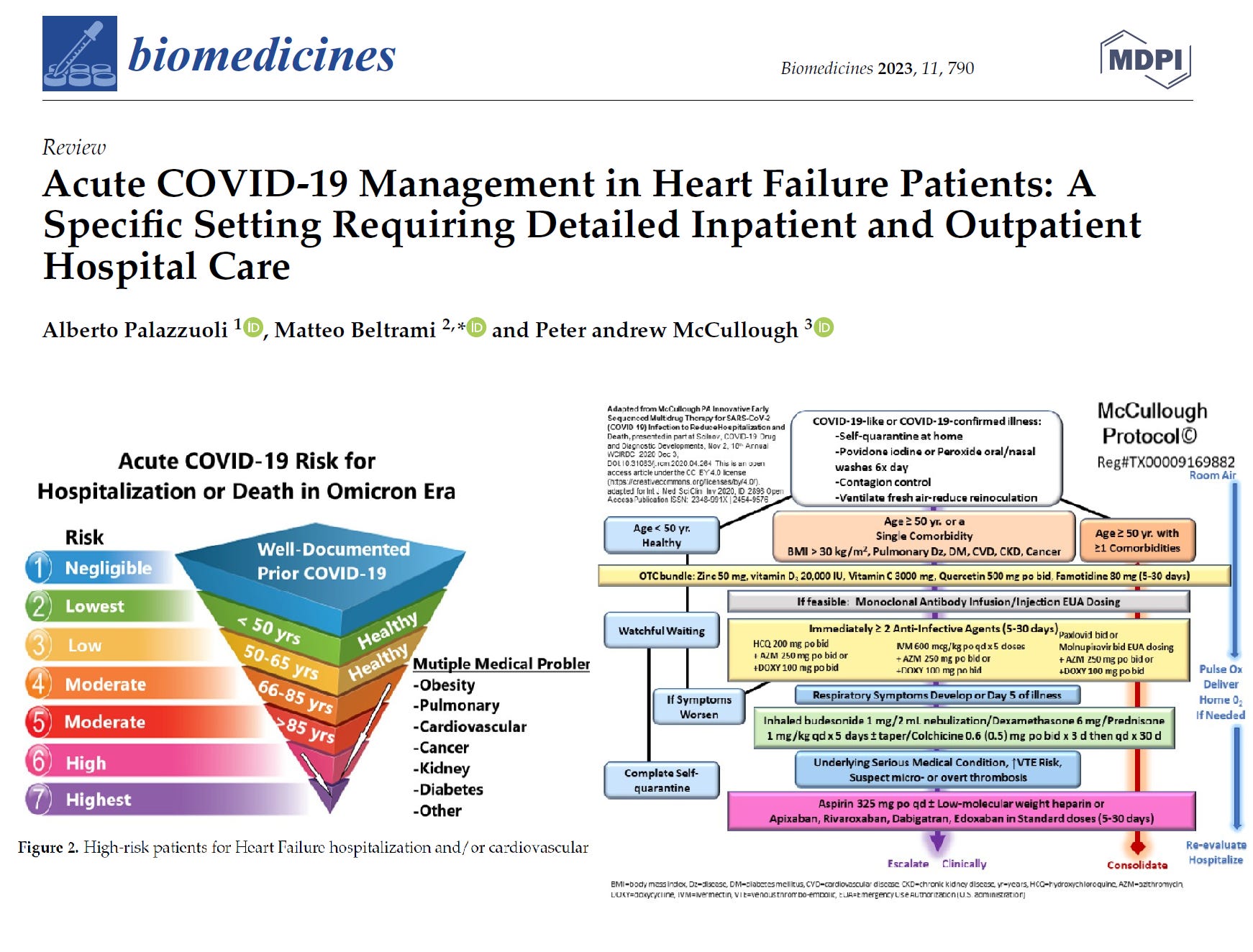
A new feature in the Palazzuoli paper is risk stratification based upon prior COVID-19 illness. A well documented case of COVID-19 during the Delta or Omicron outbreaks confers a negligible risk of hospitalization or death. This is good news and means patients and doctors should not panic and can quickly settle into a tailored home program that allows the respiratory and constitutional symptoms to be ameliorated. If hospitalization is avoided, that means complications such as ventilatory associated barotrauma, pneumothorax, nosocomial infection, contrast- or remdesivir induced acute kidney injury, hospital induced delirium, and so many other problems can be avoided.
Not shown, the paper has a select table of drugs that can be used in heart failure. Listed and safest is ivermectin, which has no drug interactions or other problems to worry about in heart failure patients. So whether vaccinated or not, when acute COVID-19 respiratory illness strikes in heart failure patients, please remember this issue of Courageous Discourse and go to the source paper by Palazzuoli et al at the link.
If you find “Courageous Discourse” enjoyable and useful to your endeavors, please subscribe as a paying or founder member to support our efforts in helping you engage in these discussions with family, friends, and your extended circles.
Dr. McCullough,
I am troubled by two aspects of the paper cited in this post. I am a layperson, so it’s possible there’s something I misunderstood or simply missed.
First, the paper says that heart patients who have received the Covid-19 injections have better hospital outcomes than those who are uninjected. You have been very clear that the so-called vaccines are dangerous and should be pulled from the market. One of your recent essays (Trial Site News, yesterday, March 5, 2023) even bemoans the fact that medical researchers seem to be blind to the fact that the Covid-19 injectables cause myopericarditis and makes the point that the injectables are inherently dangerous, saying, "The COVID-19 vaccines have caused record injuries, disabilities, and death." Yet, the comment in your paper about injected patients having better outcomes than uninjected patients could be interpreted as a plug for the very injectables you otherwise have been warning about for years. To be fair, your recent paper simply says the injectables are associated with better Covid-19 outcomes and stops short of endorsing the shots, but if you remain of the view the shots are inherently dangerous and should be pulled from the market (assuming I’ve correctly understood your position on the shots), then shouldn’t such a statement be footnoted or otherwise explained so that the reader understands that despite allegedly better outcomes among injected patients the risk profile of the shots remains so bad that the shots should be avoided by everyone? Related, we know that the medical journals and much of the data around Covid-19 has been manipulated and many now realize that medical journals (and Covid-19 data more generally) simply can’t be trusted. I wonder whether the two studies you cited in support of the statement that injected HF patients have better outcomes than uninjected HF patients are actually reliable or are part of the pervasive research fraud.
Second, the cited paper makes favorable comments about remdesivir and the McCullough treatment protocol mentioned in the paper includes molnupiravir and paxlovid among the recommended therapeutics. Before now, I’ve understood that, like the shots, all three medicines are associated with severe adverse events and very bad outcomes. Indeed, unless I’ve missed a regulatory change it’s my understanding all three are available only as EUAs, which I think suggests they haven’t gone through the full FDA approval process and there likely isn’t long term safety data to support any of them. Is there really a good reason any patient should opt for unproven EUA drugs when other fully FDA-approved medicines, like ivermectin among many others, are known to work and, as your paper says, have outstanding safety profiles?
I've been wondering how many people died of COVID outside of hospitals. I've never heard of a single case of someone dying exclusively from COVID at home.