



Antinuclear Antibody Positive Pericarditis after mRNA Vaccination
Autoimmunity Described after First Dose BNT162b2 (Pfizer/BioNTech)

By Peter A. McCullough, MD, MPH
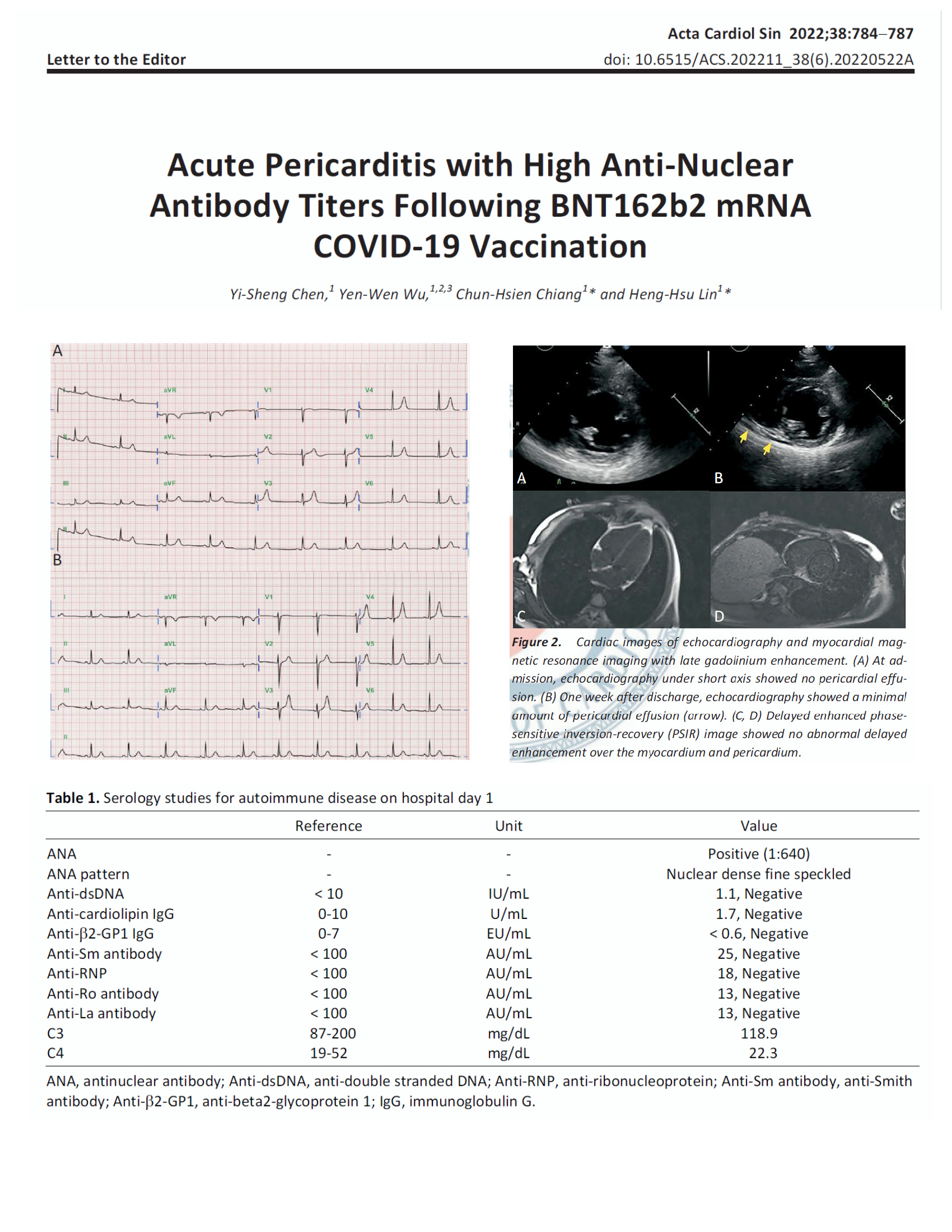
The antinuclear antibody is a well-established laboratory test to detect forms of autoimmune diseases including systemic lupus erythematosus and rheumatoid arthritis. Chen et al have described a 23 year old woman who developed pericarditis 10 days after the Pfizer vaccine. Symptoms did not resolve with colchicine and non-steroidal anti-inflammatory agents. The ANA blood test was found to be positive at a high titer. She responded well to the addition of corticosteroids.
The important point of this case is that a positive ANA can accompany COVID-19 vaccine induced myopericarditis. When it is present it may be a signal of steroid-responsiveness.
Noureldine et al have reported on 101 subjects with no history of autoimmune disease but with 18% having a family history of autoimmunity. The overall rates of positive ANA tests at low titers was the same before and after serial mRNA injections. However, in the cases where new positive tests were observed after vaccination, the specific test that turned positive was the antiphospholipid antibody which is related to blood clotting disorders.
In conclusion, there is a growing literature that mRNA and WIV Spike protein production in some recipients of genetic COVID-19 vaccines results in positive laboratory tests indicating autoimmunity. The long-term implications for emerging rheumatologic problems (pericarditis, arthritis, hepatitis) after repeated COVID-19 vaccinations are unknown. There should be a strong push to study autoimmune illnesses that emerge as a result of COVID-19 vaccination.
If you find “Courageous Discourse” enjoyable and useful to your endeavors, please subscribe as a paying or founder member to support our efforts in helping you engage in these discussions with family, friends, and your extended circles.
I have seen multiple autoimmune disorders present after mRNA jabs. However, I do not feel vindication (none of my “superiors” believed me), only a profound sadness for the affected individuals.
There is a similar situation involving my mother. After two covid shots, one booster, status post a few months after booster: Breast CA returns, (estrogen type, same previously diagnosed) radical mastectomy performed (CA returned from 12 years, in same area). My mother previously rec'd maximum round of radiation after initial CA diagnosis. After breast removed, complicated by large hematoma, which is still unresolved. My mother takes several cardiac meds. On or around 2 months s/p mastectomy, she presents with SOB and fatigue. CT scan reveals multiple blood clots bilaterally and pericarditis. She had been taking 325 mg aspirin daily for years. She has no history of valve issues, joint replacement or clotting disorders. She is not sure of why she was taking aspirin, nor were her doctors aware. A specialist is called, and after one month, the results are antibodies for Lupus at 80 years old. The cause of the blood clots are from dyscracia, caused by Lupus. She has no prior diagnosis of Lupus before this date.