




Homelessness and Hardiness to COVID-19
Toronto Study Indicates Homeless Managed Just Fine Through Pandemic

By Peter A. McCullough, MD, MPH
It is well known that homeless populations have much higher rates of hospitalization for a variety of reasons including drug abuse, alcoholism, aspiration, pneumonia, and neuropsychiatric reasons. I have always wondered how they fared during COVID-19 having heard little about severe outcomes among those who live outside.
Richard and coworkers reported on 736 homeless individuals in Toronto, Ontario during 2021 and 2022. The majority managed through the illness with no reported difficulty over the time period, most with the Omicron variants. There were no reported severe cases, hospitalizations, or deaths.
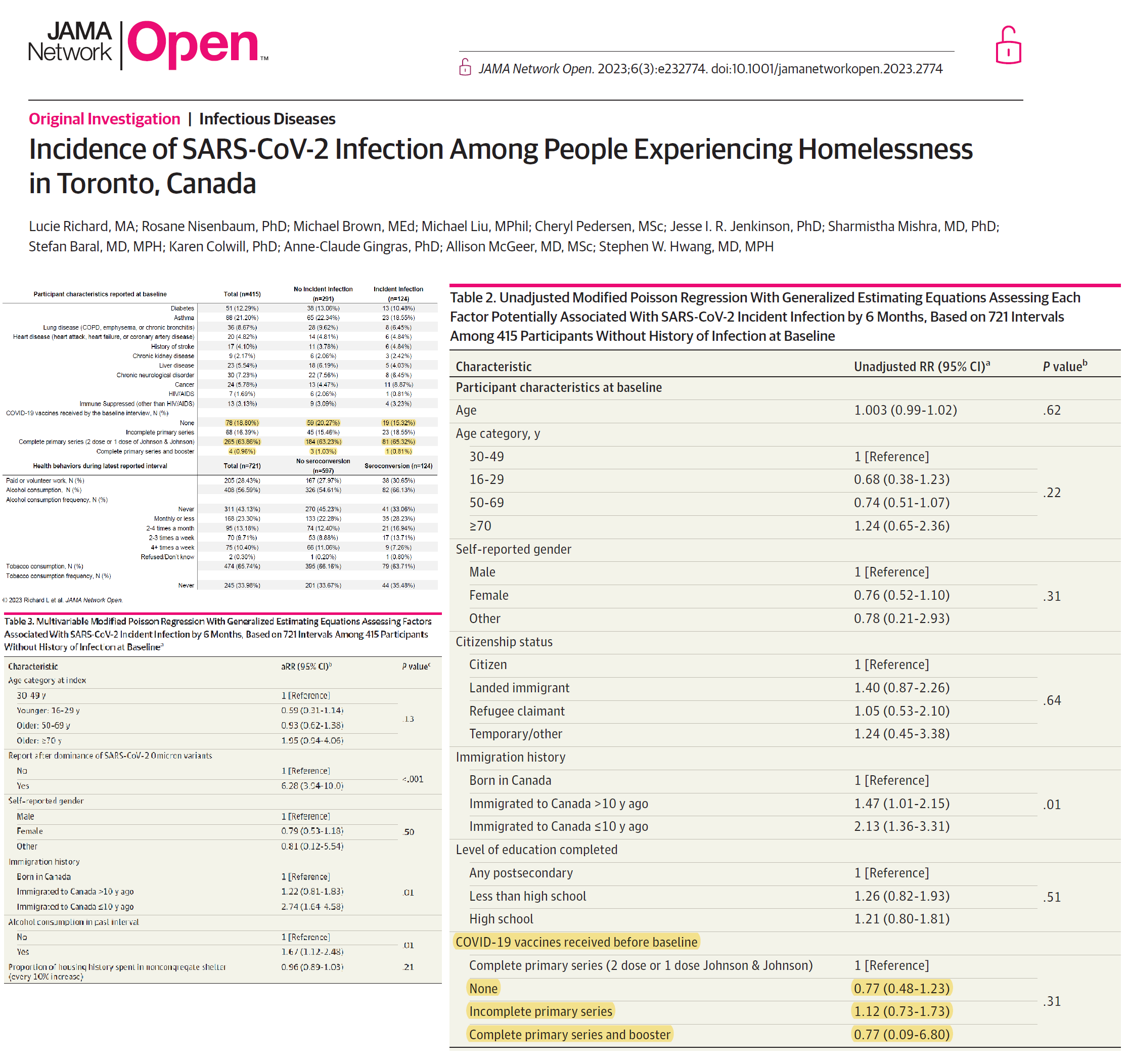
Despite approximately two thirds taking a COVID-19 vaccine, the shots appeared to be useless in this population with no statistically significant vaccine efficacy. While the public has watched the relentless pursuit of well-employed adults, college age students, and children down to 6 months of age, the most economically deprived and vulnerable in society appear to be of little interest to the Biopharmaceutical Complex, and like the other groups, have no theoretical benefit from vaccination. As a general rule if the highest risk derive no reduction in hospitalization or death, then even lower risk individuals are not worth the effort for public health interventions such as vaccines.
If you find “Courageous Discourse” enjoyable and useful to your endeavors, please subscribe as a paying or founder member to support our efforts in helping you engage in these discussions with family, friends, and your extended circles.











Arundel, writing on humidity and respiratory health, showed optimal humidity for nasal defenses at 40 to60%. That’s what is common outdoors. Living in our drier indoor environments is what causes cold season and enables pandemics.
The most obvious explanation for this is that being outside a lot more than most other people, homeless people will be more exposed to the ~297 nanometre UV-B light which converts 7-dehydroxcholesterol in their skin to vitamin D3 cholecalciferol.
This won't necessarily mean their circulating 25-hydroxyvitamin D (25(OH)D) levels are at least 50 ng/mL (1 part in 20,000,000 by mass), which is what is needed for full immune system function. However, they would, in general, have higher 25(OH)D levels than most other people who do not supplement vitamin D3. Such people usually have levels in the range 5 to 25 ng/mL, which means their innate and adaptive immune responses to cancer cells, bacteria, fungi and viruses are very much weaker (crippled) compared to what they would be with 50 ng/mL or more 25(OH)D AND they are at much greater risk of self-destructive, indiscriminate cell destroying, wildly dysregulated inflammatory responses.
Please see the research articles on vitamin D and the immune system cited and discussed at: https://vitamindstopscovid.info/00-evi/ (Co-signed by Patrick Chambers MD: https://www.researchgate.net/profile/Patrick-Chambers-4/).