



Large Korean Study Recommends Monitoring mRNA Vaccinated Patients for Auto-immunity
Modest Risks Identified, but Cumulative Effects with Repeated Boosters are Concerning

By Peter A. McCullough, MD, MPH
There is great concern that with continued dosing of mRNA COVID-19 vaccines, the human body is forced to produce not only the foreign and potentially lethal Wuhan Spike protein, but probably about a dozen additional frameshifted proteins as shown by Boros and colleagues. Invariably these peptides induce an immune attack against the human body as they are expressed on cell surfaces and in some cases like Spike protein, trimerize and are circulatory in blood for months after injection.
In clinical practice my screen for autoimmunity is through blood testing: ANA, rheumatoid factor, and anti-citrullinated peptide (anti-CCP) antibodies. If there are skin, kidney, or vasculitic features, I add the ANCA test.
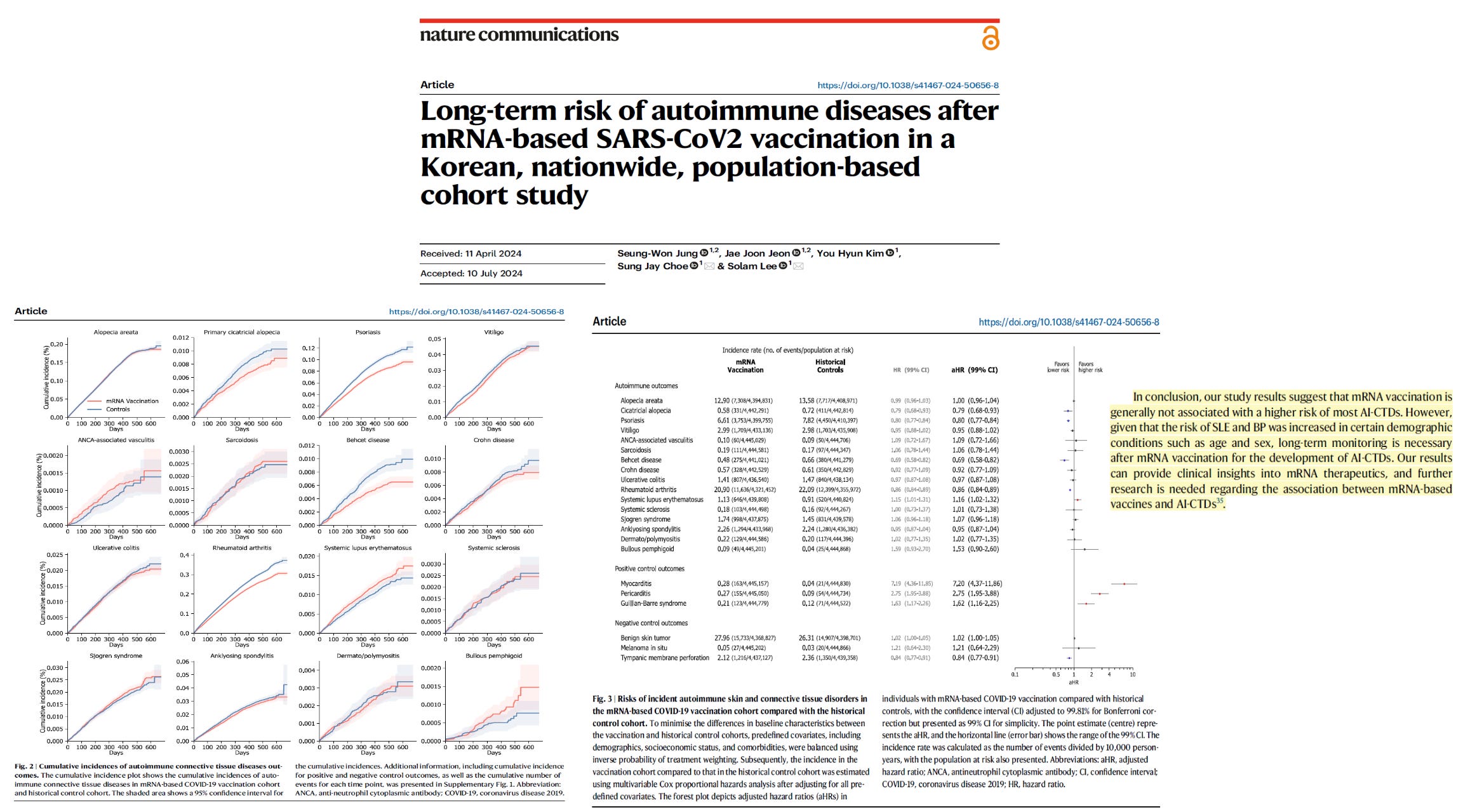
Now a large study from Korea by Jung et al, suggests there are increased risks for some autoimmune illnesses after at least two mRNA shots, but not nearly as high as the established dangers of vaccine myo-pericarditis or Guillain-Barre Syndrome.
“In this nationwide, population-based cohort study involving 9,258,803 individuals, we aim to determine whether the incidence of AI-CTDs is associated with mRNA vaccination. The study spans over 1 year of observation and further analyses the risk of AI-CTDs by stratifying demographics and vaccination profiles and treating booster vaccination as time-varying covariate. We report that the risk of developing most AI-CTDs did not increase following mRNA vaccination, except for systemic lupus erythematosus with a 1.16-fold risk in vaccinated individuals relative to controls. Comparable results were reported in the stratified analyses for age, sex, mRNA vaccine type, and prior history of non-mRNA vaccination. However, a booster vaccination was associated with an increased risk of some AI-CTDs including alopecia areata, psoriasis, and rheumatoid arthritis. Overall, we conclude that mRNA-based vaccinations are not associated with an increased risk of most AI-CTDs, although further research is needed regarding its potential association with certain conditions.”
Because these diagnoses are based on laboratory tests, Jung and coworkers may have underestimated incidence since not all vaccinated patients get laboratory monitoring in follow-up. Jung concluded: “long-term monitoring is necessary after mRNA vaccination for the development of autoimmune connective tissue diseases.” These data suggest however, I could reduce the intensity of screening for auto-immunity and make it more clinically directed based upon symptoms. When auto-immunity is found, the most common drug I use in my practice is hydroxychloroquine. However, I have had advanced cases that have required methotrexate, prednisone, and even rituximab. Media star Megyn Kelly serves as an example of this very real vaccine hazard.

Please subscribe to Courageous Discourse as a paying ($5 monthly) or founder member so we can continue to bring you the truth.
Peter A. McCullough, MD, MPH
President, McCullough Foundation
Consider the risks to a patient already suffering from multiple autoimmune disorders. Our youngest
Thank you, Dr McCullough. I appreciate the hard work that you put in and your foundation! I am a proud Founder Member and think that this is a good investment in decent science and quality information!