



Safety Reporting of COVID-19 Vaccine Induced Myocarditis
Just Seeing the Tip of the Iceberg

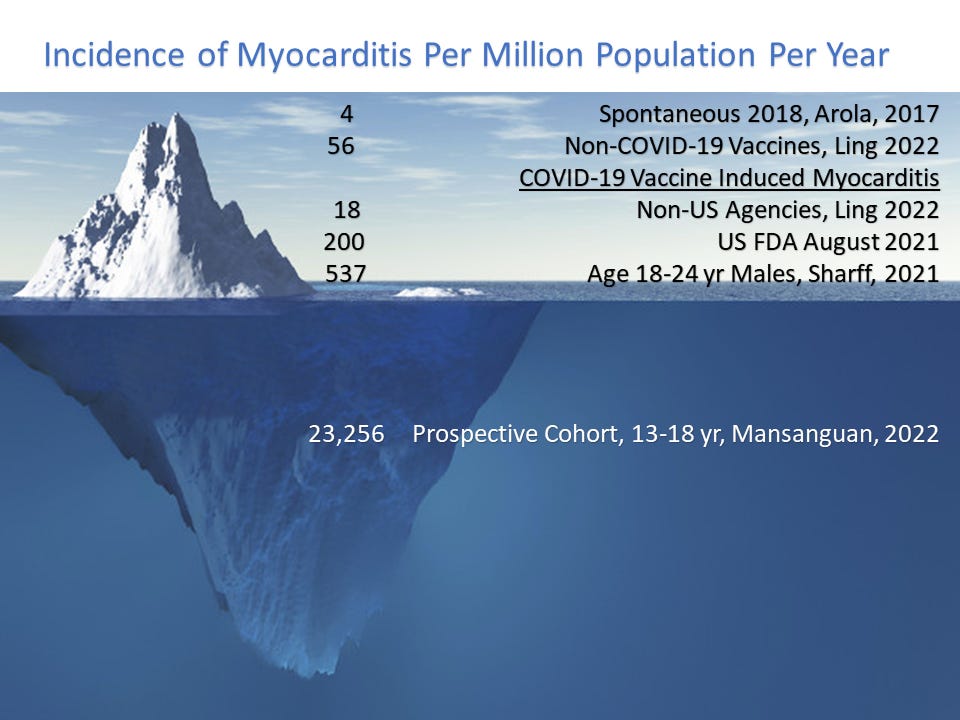
In 2021 the US CDC and FDA warned America and the world that the mRNA COVID-19 vaccines could result in heart inflammation or myocarditis.[i] This is a medical problem that has occurred in the past not related to vaccines but at a low rate ~4 per million population per year as reported by Arola, et al, from Finland. In general, ~90% of cases occur in men and ~10% in women.[ii] The principles of management include stopping all forms of exercise since that can be a driver of the development of heart failure and a trigger for sudden death. In cases where there is a progression to heart failure, cardiac biopsy is commonly performed to establish or rule out a diagnosis of giant cell myocarditis which has a markedly worse prognosis than the other forms (parvovirus, etc). COVID-19 vaccination has been thrust on the world with such vehemence that there has been a hesitancy among physicians and hospitals to spontaneously report cases to the regulatory agencies. The vast majority of physicians took COVID-19 vaccines themselves and may be having trouble coming to personal grips with the threat of heart damage and other risks of vaccination. In 2021 as spontaneous reports came into agencies that predominately young men were developing myocarditis with COVID-19 vaccination, a pattern emerged: 1) highest risk group was males age 18-24 with a skewed distribution and a long tail that extended to men in their seventies, 2) ~90% of required hospitalization, 3) risk was explosive after the second injection, 4) death directly due to myocarditis was confirmed by autopsy. In the biological licensing agreement letters to Pfizer and Moderna, the US FDA requested prospective cohort studies of myocarditis which call for measurement of blood tests, ECG, and cardiac imaging before injections and at timepoints afterwards to detect the real rate of heart damage and to ascertain how much of the problem could be asymptomatic and potentially present a future risk of sudden death in an unsuspecting patient. Both companies were not forthcoming, so the answer came from Mansanguan et al, from the Bhumibol Adulyadej Hospital, Bangkok, Thailand.[iii] Adolescents age 13-18 were studied in a prospective cohort manner just after the second injection of the Pfizer vaccine and 7/301 (23,256/million) developed myocarditis using a clinical definition based on blood tests, ECG, and cardiac imaging. Data from multiple sources suggest the condition can be subclinical in about half, meaning neither the patient nor the parents bring it to clinical attention. Patone et al have recently reported on 100 fatal cases of vaccine-induced myocarditis in the UK, and such papers are expected to continue with larger numbers as the medical community begins to fully recognize cause and effect.[iv] Thus spontaneous reporting to agencies represents the tip of a very large iceberg.
If the estimate Mansanguan study is confirmed or anywhere close to ~25,000/million, that means a million young Americans could have sustained heart damage from COVID-19 vaccination and some of them will be at risk for cardiac arrest and future heart failure. These data suggest we should not be surprised by rising rates of sudden death in young persons with sports and during daily life including sleep. There can be no more urgent need to halt vaccination and commit a substantial research effort into screening, detection, prognosis, and management of COVID-19 vaccine induced myocarditis. The stakes are high—an entire generation is at risk.
[i] FDA Summary Basis for Regulatory Action, Nov 8, 2021
[ii] Arola A, Pikkarainen E, Sipilä JO, Pykäri J, Rautava P, Kytö V. Occurrence and Features of Childhood Myocarditis: A Nationwide Study in Finland. J Am Heart Assoc. 2017 Nov 18;6(11):e005306. doi: 10.1161/JAHA.116.005306. PMID: 29151030; PMCID: PMC5721735.
[iii] Mansanguan S, Charunwatthana P, Piyaphanee W, Dechkhajorn W, Poolcharoen A, Mansanguan C. Cardiovascular Manifestation of the BNT162b2 mRNA COVID-19 Vaccine in Adolescents. Trop Med Infect Dis. 2022 Aug 19;7(8):196. doi: 10.3390/tropicalmed7080196. PMID: 36006288; PMCID: PMC9414075.
[iv] Patone M, Mei XW, Handunnetthi L, Dixon S, Zaccardi F, Shankar-Hari M, Watkinson P, Khunti K, Harnden A, Coupland CAC, Channon KM, Mills NL, Sheikh A, Hippisley-Cox J. Risk of Myocarditis After Sequential Doses of COVID-19 Vaccine and SARS-CoV-2 Infection by Age and Sex. Circulation. 2022 Sep 6;146(10):743-754. doi: 10.1161/CIRCULATIONAHA.122.059970. Epub 2022 Aug 22. PMID: 35993236; PMCID: PMC9439633.
The proportion of reports mentioning "Troponin increased" and/or "Myocarditis" in 15-17 year old double vaccinated boys who had a COVID infection is over 33%.
http://pervaers.com/img/myocarditis_troponin_increased.png
Myocarditis as a product of vaccine induced coronavirus disease enhancement
Difference in proportion of reports from male patients 12-17 compared to other vaccines:
+0.372% (shot 1 without infection)
+6.339% (shot 2 without infection)
+11.785% (shot 1 with infection
+15.565% (shot 2 with infection)
https://pervaers.com/?v=c10&q=_myocarditis_
https://pervaers.com/?v=c11&q=_myocarditis_
https://pervaers.com/?v=c20&q=_myocarditis_
https://pervaers.com/?v=c21&q=_myocarditis_
And we know it's not the illness itself: https://pubmed.ncbi.nlm.nih.gov/35456309/
This effect does not occur in pericarditis, only myocarditis.
It is even more pronounced for the medical concept "Troponin increased". I've also noticed it applies to "Acute kidney injury", probably to a lot of other concepts as well.
This will list all cardiac signals for covid vaccines, limited to reports without infection:
https://pervaers.com/?vax=cc0&q=*cardiac
This will list all cardiac signals for covid vaccines, limited to reports with infection:
https://pervaers.com/?vax=cc1&q=*cardiac
I explain my methodology in detail in the help section (https://help.perVAERS.com), but it's pretty basic for people with good knowledge of statistics.