



A Prospective Study of the Incidence of Myocarditis/Pericarditis and New Onset Cardiac Symptoms following Smallpox and Influenza Vaccination
Spontaneous Reporting Grossly Underestimates True Incidence

By Peter A. McCullough, MD, MPH
We have been barraged by government agency statements and peer-reviewed publications from academic medical centers asserting that serious complications from COVID-19 vaccination are “rare.” Often, investigators take a number of spontaneously reported events from a data system, and in error, divide that number by the total injections given in a period of time. This is incorrect since not all individuals who took the vaccine were assessed for the outcome and we cannot assume they are OK.
Engler et al from Military Vaccine Agency-Vaccine Healthcare Centers Network (currently Defense Health Agency, Immunization Healthcare Branch), make this point with an analysis of myocarditis after smallpox and trivalent influenza vaccination. Both study cohorts were evaluated during a pre-immunization visit and up to 2 post-vaccine visits (day 5–8 and/or day 9–28). Baseline data including age, race/ethnicity, sex, cardiac risk factors, atopic/medical history, and fitness assessments as measured by physical training abilities, were collected on the day of the SPX or TIV immunization. Clinical data including cardiac symptoms with visual analogue scale rating (0–10) of severity, 12-lead electrocardiograms (ECG), and troponin-T were collected at baseline and at between days 5 and 30.
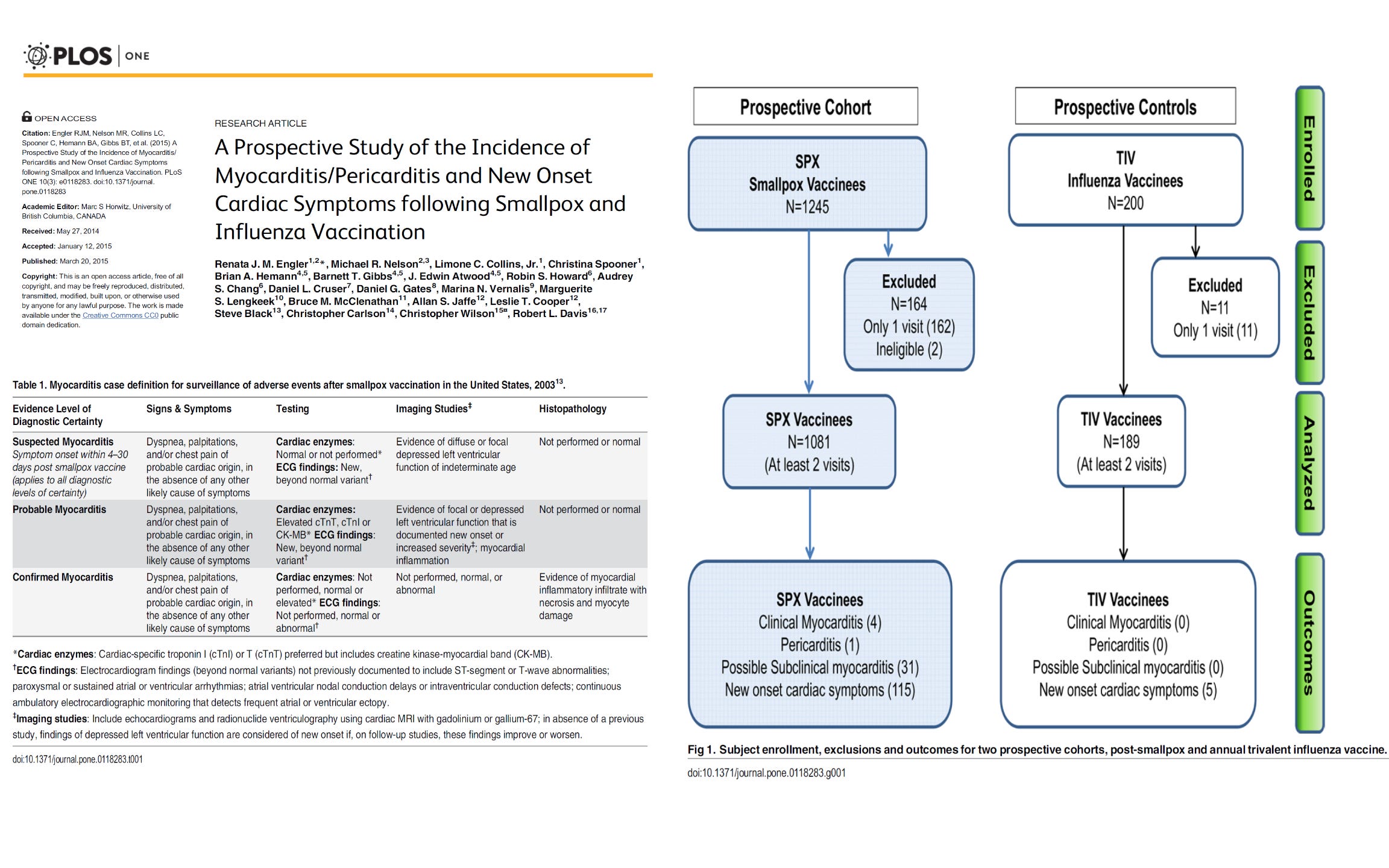
While there were no myopericarditis events with the influenza vaccine, there were 5 cases with the smallpox shot. Compared to historical rates of spontaneous reporting, there was a fourfold increased incidence of cardiac symptoms when assessed prospectively.
In vaccine safety research, we should not trust any assertions of “rarity” unless it is a prospective cohort study in which all recipients are checked. We should focus on the absolute number of serious adverse events which are the crude data. These numbers cannot be argued with our understanding that they indeed happened, but are likely to be a gross underestimate of reality.
If you find “Courageous Discourse” enjoyable and useful to your endeavors, please subscribe as a paying or founder member to support our efforts in helping you engage in these discussions with family, friends, and your extended circles.
Dr Mc cullough. Can you please do a substack for your subscribers on what tests should be done to look for subclinical myocarditis? We just got word last night that my brother in law “died suddenly”. I’ve urged his wife to have an autopsy done because his grown children took the shot as did some of my children and family that are healthcare professionals. As you know we can’t trust our own doctors because they deny the connection. So what tests should be done as a precaution? Thanks in advance. We are all in shock. I fear it was that shot.
I appreciate how you've pointed out that no endpoint assessment was done on all recipients of the genetic "therapy" injection, ergo it is impossible to assume that issues were confined to those who reported problems. This very likely skews the statistics (which are already horrific, compared to historical records for the other vaccines). And the regular vaccines are no "walk in the park" themselves, as the timeline for rocketing autism rates suggest a correlation to bloated childhood vaccine schedules. We already know from one CDC whistleblower that the agencies have colluded with industry to cover up harm in the past, so it leaves one wondering what else did they do that hasn't yet come to light?