


Circulating Spike Protein that Evades Antibodies
Circulating Spike Protein that Evades Antibodies
Understanding Determinants of COVID-19 Vaccine Induced Myocarditis

By Peter A. McCullough, MD, MPH
One of the toughest questions I had on my interview with Joe Rogan in 2021 was “Dr. McCullough, if the COVID-19 vaccines are so bad, how come everybody doesn’t die after taking them?” While as naïve and ridiculous as it sounds, its a good question and brings up the goal of epidemiology: to study of the distribution and determinants of disease. Roughly 15% of vaccine recipients develop a health problem after taking a COVID-19 vaccine (Zogby, 2022) based on the lot number (proxy for mRNA quantity or contaminants), susceptibility, and pre-existing disease (e.g. inherited blood clotting disorder). No young person should be hospitalized after taking a COVID-19 vaccine since that outcome far outweighs any theoretical benefit of the injections.
Massachusetts General Hospital, Harvard School of Medicine, had 13 young boys and 3 girls hospitalized with myocarditis and available for study. Yonker et al found all the subjects had large quantities of free circulating Spike protein generated from the vaccines while control subjects without myocarditis did not.
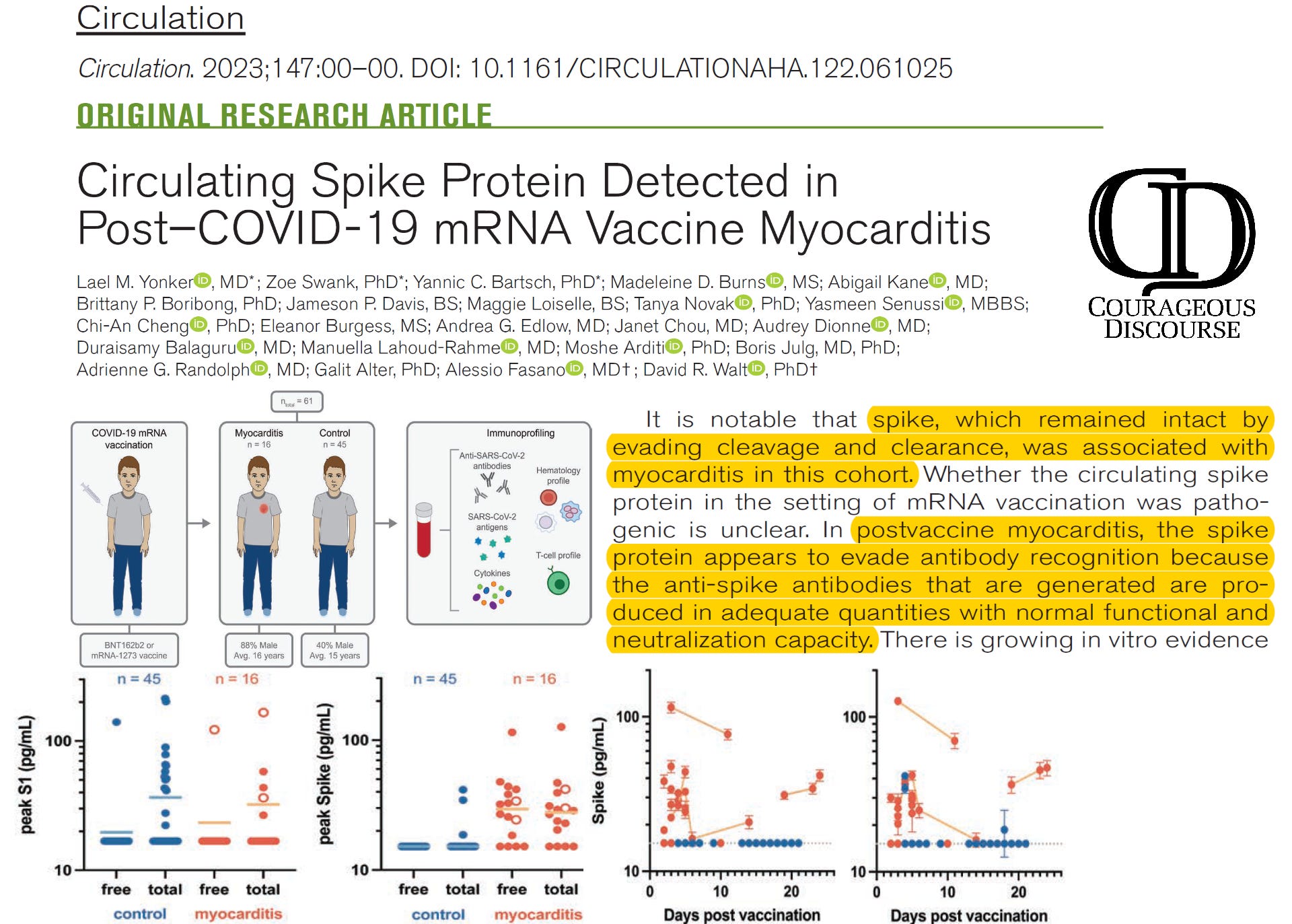
The Spike protein they had evaded the apparently sufficient library of antibodies that were supposed to neutralize it. Thus, it is possible that some persons do not make specific neutralizing antibodies after injection, and thus, the Spike protein is able to circulate and damage the body, specifically the heart muscle. The race is on to develop commercialized Spike protein tests and possibly monoclonal antibodies against the vaccine-induced Spike that could neutralize it and prevent more heart damage. It is ironic that our government quickly pulled monoclonal antibodies off the market for anticipated lack of efficacy with new strains and now these products could be useful against the legacy Spike protein produced by the ill-conceived COVID-19 vaccines. Clearly more research is needed. This “positive” paper on the pathophysiology of COVID-19 vaccine induced myocarditis should spur more research on thousands of young persons now suffering with heart damage from the vaccine debacle.
If you find “Courageous Discourse” enjoyable and useful to your endeavors, please subscribe as a paying or founder member to support our efforts in helping you engage in these discussions with family, friends, and your extended circles.
Peter, rather than postulating differential responses of spike protein manufacturing in different COVID-19 vaxx recipients, I think it more likely that the vaccines themselves differ one from the next in their capacity to cause the body to produce spike protein. This theory is consonant with the www.howbadismybatch.com data which demonstrates that different batches had different adverse event rates. These phenomena suggest the obvious: that good manufacturing principles were not followed by the vaccine makers, and that therefore some batches contained far more mRNA than others. There is some evidence that the manufacturers were aware of the toxic batches, and rather than withdrawing them from the market, they distributed them widely across the country in a deliberate attempt to obscure the harm, which would have been glaringly apparent had the bad batches been confined to local distribution.
"Thus, it is possible that some persons do not make specific neutralizing antibodies after injection, and thus, the Spike protein is able to circulate and damage the body, specifically the heart muscle." It seems that for vaccines to be effective a properly functioning immune system is needed, More immune system research is needed and maybe vaccines could be eliminated if the immune system was functioning properly. There has not been a pandemic yet that killed everyone. Those with good immune systems survived. We have to get a better understanding of what is needed to have an immune system that can rise to any challenge.