



Rubella--The Most Compelling Component of MMR
German Measles Vaccine Has Protected Against Congenital Rubella Syndromes

By Peter A. McCullough, MD, MPH
When the CDC added the genetic EUA COVID-19 vaccines to the expanding routine childhood schedule in 2022, it triggered a reappraisal of the common vaccine combination products. In prior sub stacks I have pointed out that there are clear breakthrough cases of measles and mumps in fully vaccinated individuals. These outbreaks suggest the vaccines do not fully prevent disease occurrence or transmission, however their wide deployment has been associated with a reduction in sporadic cases and sequalae worldwide. Fortunately modern medical care for those who develop disease is a far more important determinant of survival than a vaccine taken years ago. Thus I advise vaccine proponents to refrain from the conclusion that vaccines save lives, since it is really supportive care that would save a life of a patient vaccinated or not who develops critical illness.
Rubella (German measles, 3-Day measles) virus is a single-stranded RNA virus with spike-like, hemagglutinin-containing surface projections. In a woman of childbearing potential, rubella can cause fetal loss or severe birth defects in up to 90% of cases. The rubella vaccine is very effective in preventing maternal Rubella, but the women must be vaccinated before pregnancy.
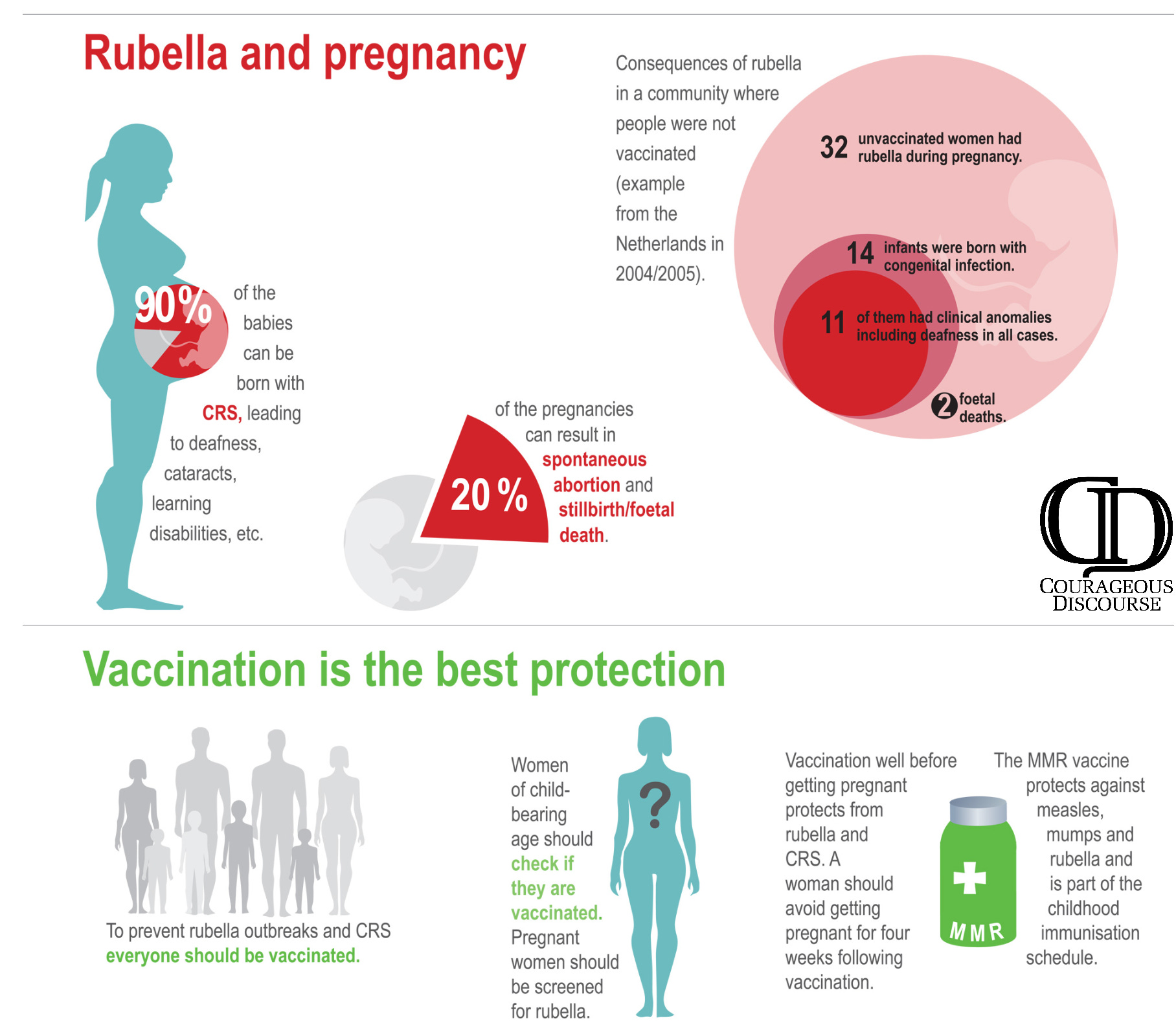
Rubella in children is either asymptomatic or a mild self-limited illness. The public health strategy has been to mass vaccinate the entire childhood population to prevent kids and young adults from passing it to the pregnant mother and hopefully have provided direct protection of the mother with antecedent vaccination. Maternal protection can be assessed by antibody titers.
The CDC says the live attenuated Rubella vaccine is 97% effective. “The last major epidemic in the United States occurred during 1964 to 1965, when there were an estimated 12.5 million rubella cases in the United States. Because of successful vaccination programs, rubella has been eliminated from the United States since 2004.” The CDC goes on to indicate: “Today, less than 10 people in the United States are reported as having rubella each year. Since 2012, all rubella cases had evidence that they were infected when they were living or traveling outside the United States. To maintain rubella elimination, it is important that children and women of childbearing age are vaccinated against rubella.” Thus the strategy of mass indiscriminate vaccination works for rubella.
For discerning parents the question is: Does every child need a Rubella vaccine or just girls before they enter the childbearing years of their lives? There are sporadic cases of self-limited vaccine induced Rubella in the immunocompromised and immunocompetent. Dr. Best in 2007 wrote: “Countries should ensure that susceptible women of child-bearing age and health care workers are offered a rubella-containing vaccine.” She was suggesting in some countries with limited resources, that a targeted approach could be taken.
As an internist and cardiologist I am fielding questions on vaccines daily since the COVID-19 vaccine debacle. In my view the rubella component has been the strong suit of MMR. In the future, targeting the rubella vaccine to the group with medical necessity that is women of childbearing potential could be considered. It would be nice to see a shot in the arm that was so effective in blocking a nasopharyngeal respiratory infection, that we would not have to inject hundreds of millions of people who truly have no clinical indication in an attempt to “herd protect” a subsegment of the population.
If you find “Courageous Discourse” enjoyable and useful to your endeavors, please subscribe as a paying or founder member to support our efforts in helping you engage in these discussions with family, friends, and your extended circles.
That used to be the case. At the age of 13 in the UK girls were tested and if they hadn't already had rubella, we were vaccinated against it. Given the risks of rubella in early stage pregnancy I supported that and was vaccinated. What I don't understand is why would you give it with mumps and measles and to a baby. The key point is that for healthy children these childhood diseases not only weren't a problem but helped provide a strong immune system through adult hood. I had measles as a child - apart from the rash, I wasn't ill.
Childhood illnesses were a problem for vulnerable children as were all infections. The DTP vaccine was a classic example of transferring risk from vulnerable children to healthy children. There was no reduction in deaths, just different children were dying ie those vaccinated. Which was why once the evidence of the harm of the pertussis vaccine came out I didn't vaccinate my children. Sir Gordon Stewart's work explained and provided the evidence for what was going on. A very fine epidemiologist and public health officer, he was later vilified as anti-vaccine. Tragically 'twas ever thus.
When applying for a new clinical position in 2020 the hospital required Ab titres for measles, mumps, and varicella all of which diseases I had as a child about 60 years ago and Hepatitis B which I was vaccinated for in the Army about 30 years ago. The antibody levels for MMR were 20 to 1000 times the level demonstrating immunity while the Hep B was just barely adequate. I never considered myself anti vaxx but Covid led me to examine what I thought I knew about vaccines. Given the risks, lack of effectiveness and mostly benign course for these childhood diseases I think it’s time for new approach.