



SARS-CoV-2 Spike Protein Causes Blood Clots
It is at the Scene of the Crime

By Peter A. McCullough, MD, MPH
One of the remarkable observations about SARS-CoV-2 infection is the clinical manifestation of venous and arterial thrombosis. Multiple studies have described thrombotic complications of the infection including stroke, myocardial infarction, systemic arterial embolism, and deep venous thrombosis with pulmonary embolism. In my practice I have seen virtually every one of these complications. De Michele and colleagues studied patients with COVID-19 in 2020, before there were vaccines for the population.[i]
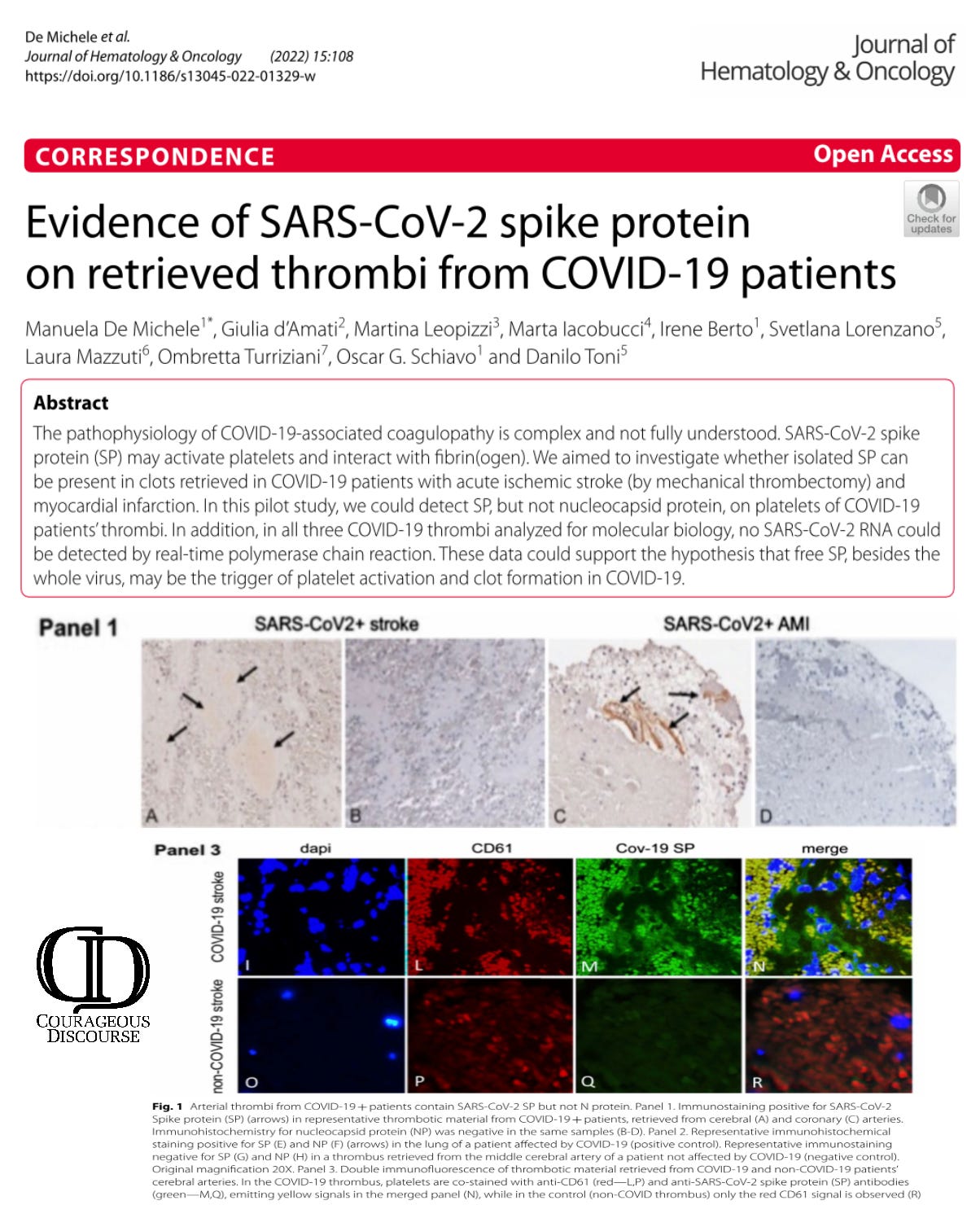
They found SARS-CoV-2 Spike protein directly attached to platelets within the blood clots retrieved from patients. Importantly, there was no evidence of the entire virus. This suggests the Spike protein disassociates from the virus and becomes its own clot forming missile within the human body. I could anticipate that mRNA, adenoviral DNA, and Spike protein antigen-based vaccines act the same way by generating free Spike protein within plasma which is able to circulate and participate in the development of blood clots. Virchow’s triad is an axiom in medicine that says blood clots require three elements: 1) injury to the vessel wall,[ii] 2) stasis of blood, and 3) a hypercoagulable state. SARS-CoV-2 Spike protein is known to damage the endothelial lining of capillaries and blood vessels and cause hypercoagulability. Stasis of blood is inherent in various venous beds such as the cavernous sinus of the brain, portal vein in the abdomen, pelvic veins, and in the lower extremities of immobilized patients. Thus for venous thromboembolic cases Virchow’s triad is fulfilled. The arterial emboli take more explanation suggesting atherosclerotic plaque instability, platelet aggregation, and Spike protein driven hemagglutination, fibrin deposition, and progressive clot formation occur. No matter what the sequence, in the setting of SARS-CoV-2 infection, blood clots can be attributed to Spike protein. Large questions remain: 1) for how long after infection can Spike protein trigger atherosclerotic cardiovascular events (heart attack and stroke) and venous thromboembolism? 2) what is the initial risk period and accumulated risks of additional infections and or COVID-19 vaccination? 3) what are the best methods for screening, detection, diagnosis, prognosis, and management?
If you find “Courageous Discourse” enjoyable and useful to your endeavors, please subscribe as a paying or founder member to support our efforts in helping you engage in these discussions with family, friends, and your extended circles.
[i] De Michele, M., d’Amati, G., Leopizzi, M. et al. Evidence of SARS-CoV-2 spike protein on retrieved thrombi from COVID-19 patients. J Hematol Oncol 15, 108 (2022). https://doi.org/10.1186/s13045-022-01329-w
[ii] Zhang J, Tecson KM, McCullough PA. Endothelial dysfunction contributes to COVID-19-associated vascular inflammation and coagulopathy. Rev Cardiovasc Med. 2020 Sep 30;21(3):315-319. doi: 10.31083/j.rcm.2020.03.126. PMID: 33070537.
Pretty early in 2020, my then 76yo mother, an RN at a nursing home in PA, came down with the Rona. With hx of stroke and COPD, "her daily menu" of meds consisted of Plavix, an ACE inhibitor, a beta blocker, several corticosteroid inhalants, and PRN nebs for home use. My brother, an Interventional Cardiologist, was pushing me (by phone) to bring her to the hospital, and like any good ED RN, I pushed back and prevailed. We kept her home, and I nebbed the crap out of her, but she did pretty well. What still kills me is that my brother, who did med school and residency in the 90s and early 2000s while I was working my Level 1 Trauma/university hospital circuit, bought into the lie entirely. He is still stumped as to why he is cathing such young patients. After his 2nd Moderna shot, he had to be treated for new onset afib. Of course, I suggested the jab was most likely responsible for his AF; he scoffed and told me, "No. Alcohol and altitude." as he happened to be on a ski trip in Vail. What is with the complete and total brain shut off amongst physicians?
This is exactly why, when my family contracted the virus, we used the FLCCC protocol which called for a full aspirin a day to prevent clots. We ranged in ages from 6 months to 70 years old - and I am pre-diabetic and heavy - we were all fine - 6 of us are unvaxed and we were all equally ill and we all were fine - no clots, no long haul covid. the book is excellent - I've read it more than once to hone up on my knowledge.